| ||||||||||
| ||||||||||
Care for the dying is often a powerful illustration of treatment going too far.
Texas author Liza Ely had lined up hospice care for her 93-year-old mother, Verna Burnett, as she lived her last days with Alzheimer's and heart failure. Yet when Burnett developed an irregular heartbeat, the care provider at her Tyler, Texas, nursing home recommended seeing a cardiologist, to have a tube threaded through blood vessels to her heart to check it out.

"We were speechless," Ely said. "We asked what could be done if something showed up on the test."
The response: "Nothing, really."
Ely said the family refused the "painful, expensive and unnecessary test."
Congress' health care overhaul initially included a provision that would have authorized Medicare to pay doctors for counseling patients interested in end-of-life options. The provision died in the hue and cry after Sarah Palin dubbed the effort "death panels," a charge named 2009 political "Lie of the Year" by the nonpartisan fact-checking organization PolitiFact.
Rep. Earl Blumenauer, D-Ore., said he plans to reintroduce his idea.
"Today there is no guarantee that people will get the care they want when they are incapacitated or in those final stages of life. The default is sometimes the most painful, the most intrusive, the most frightening treatment -- whether or not that is what people want," he told the AP.
___
New efforts are beginning to push back against overtreatment:
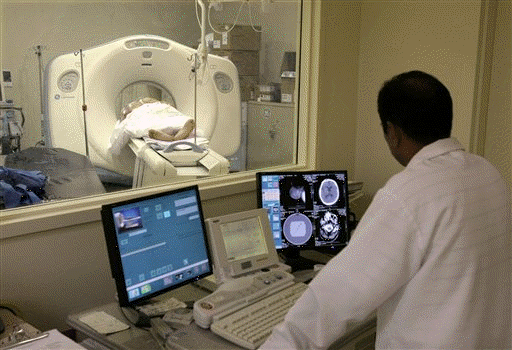
In Minnesota, the influential health cooperative HealthPartners saw use of MRIs and radiation-heavy CTs growing between 15 percent and 18 percent a year. So the insurer began a new program: National radiology guidelines pop up on each patient's electronic medical record whenever a doctor orders a scan. It's not a requirement, but a gentle reminder of when such tests are recommended.
In two years and counting, HealthPartners estimates it avoided 20,000 unnecessary tests, preventing dangerous radiation exposure and saving $14 million.
Providing the guidelines helps doctors deal with patients who demand a scan, says medical director Dr. Pat Courneya. He recently examined a young man who wanted a brain CT because of dizziness. Courneya's physical exam turned up no neurologic red flags like weakness or eye problems, but seeing the guidelines helped reassure the man.
An American Medical Association journal, Archives of Internal Medicine, just began a "Less is More" series to educate doctors about the risks of overused treatments.
First up: Studies saying more than half of the 100 million-plus prescriptions for the strongest stomach acid suppressors
-- proton pump inhibitors such as Nexium -- go to people who don't need something that powerful. That puts them at unnecessary risk of side effects, including bone fractures and infections.
This summer, the journal Annals of Internal Medicine begins publishing American College of Physicians' guidelines for "high-value, cost-conscious care."
To increase patients' savvy, about a dozen health centers around the country are testing "shared decision-making." That process uses plain-English guides, often DVDs, to explain the advantages and disadvantages of test and treatment options. Given full information, patients choose a less aggressive approach than doctors initially recommend about 20 percent of the time, says Dr. Michael Barry of the nonprofit Foundation for Informed Medical Decision-Making.
"Where I think no one in the Consumer Reports age would go to the car lot and say,
'I'm going to let the dealer figure out what car I want or need,' now we are taking a little of that spirit to the doctor's office," he said.

___
Online:
American College of Physicians:
http://www.acponline.org/
National Quality Forum:
http://www.qualityforum.org/
American Medical Association:
http://www.ama-assn.org/
National Institutes of Health:
http://www.nih.gov/
Dartmouth Institute for Health Policy:
http://tdi.dartmouth.edu/
Dartmouth Atlas of Health Care:
http://www.dartmouthatlas.org/
American College of Emergency Physicians:
http://www.acep.org/
HealthPartners:
http://www.healthpartners.com/public/
Archives of Internal Medicine:
http://archinte.ama-assn.org/
Foundation for Informed Medical Decision-Making:
http://www.informedmedicaldecisions.org/
Annals of Internal Medicine:
http://www.annals.org/
[Associated
Press;
Copyright 2010 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.


News | Sports | Business | Rural Review | Teaching & Learning | Home and Family | Tourism | Obituaries
Community |
Perspectives
|
Law & Courts |
Leisure Time
|
Spiritual Life |
Health & Fitness |
Teen Scene
Calendar
|
Letters to the Editor