| ||||||||||
| ||||||||||
Was all her testing overkill, or good care?
Moore said she wouldn't second-guess the doctors. "They went to school for it, they should know," she said.
Schaider said the CT scan was needed to rule out appendicitis or an infection, but above all to exclude any emergency, life-threatening condition. "That's our No. 1 thing," Schaider said.
He dismissed the idea of overtesting. "We do what testing we think is necessary," he said. "Most of the time we're really motivated by what benefits the patients most."
Still, he said lawsuit concerns play a role in testing decisions at ERs in publicly funded hospitals like Stroger, too.
Missed heart attacks like Stacy Meaux's are the top reason patients sue emergency doctors
The 41-year-old Texas woman sought emergency treatment for chest pain at Christus St. Mary Hospital in Port Arthur, Texas, but doctors didn't think it was heart-related and sent her home. She fell dead of a heart attack several hours later. Her family won a malpractice lawsuit in January.
Meaux was overweight, with high blood pressure and diabetes when she died Oct. 3, 2007. Doctors did two electrocardiograms -- a heart test using little sensors placed on the chest and elsewhere. They also checked Meaux's blood pressure, but skipped other heart tests, and sent her home with medicine for high blood pressure and asthma-like symptoms, court documents show.

A jury found Meaux's doctor and the hospital negligent and awarded her family more than $1 million in damages. A hospital spokesman said he couldn't comment because the hospital is appealing the verdict.
Meaux's mother, Mary Ann Licatino, isn't so worried about ER overtesting.
"I just don't have any faith in emergency rooms, because I lost a daughter," Licatino said. "They're not doing enough."
However, as many as 95 percent of ER patients with chest pain aren't having a heart attack, so it's more typical that doctors go overboard with testing.
"Often we are testing for that 5 percent," said Dr. Rahul Khare, an emergency physician at Northwestern Memorial Hospital in Chicago.
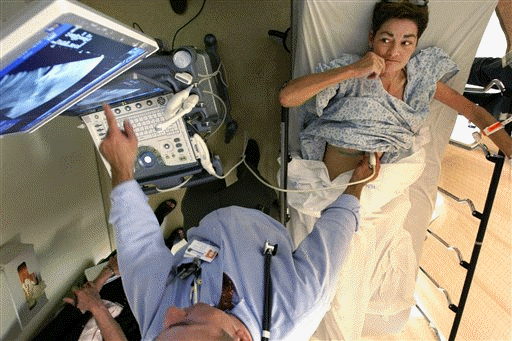
Patients with suspected heart attacks often get the range of what the ER offers, from multiple blood tests that can quickly add up in cost, to X-rays and EKGs, to costly CT scans, which are becoming routine in some hospital ERs for diagnosing heart attacks.
Costs vary. At Northwestern, a heart CT scan runs roughly $900, Khare said. Add bloodwork, chest X-ray and EKGs and the total easily approaches $2,000.
And the battery of testing may be paying off: A few decades ago insurance statistics showed that about 5 percent of heart attacks were missed in the emergency room. Now it's well under 1 percent, said Dr. Robert Bitterman, head of the American College of Emergency Physicians' medical-legal committee.
"But you still get sued if you miss them," Bitterman added.
Audrey Vernick of Ocean Township, N.J., knows that doctors sometimes overtest. But she also understands their dilemma.
"They're so scared of not catching what might be there," Vernick said. "I can so see both sides of it."
Vernick's 10-year-old daughter, Anna, twisted her ankle in gym class last fall and Vernick couldn't get an appointment with an orthopedic specialist. So she took Anna to the ER just to be safe -- a visit that cost about $1,000. The family's insurance covered it.
Anna was limping but could walk and her ankle wasn't swollen or excruciatingly painful. Common guidelines say those symptoms suggest a fracture is unlikely and an X-ray is unneeded. She got one anyway.
It showed the ankle wasn't broken.
___
Online:
National ER data:
http://www.cdc.gov/nchs/data/nhsr/nhsr007.pdf
American College of Emergency Physicians:
http://www.acep.org/
[Associated
Press;
Copyright 2010 The Associated Press. All rights reserved. This material may not be published, broadcast, rewritten or redistributed.


News | Sports | Business | Rural Review | Teaching & Learning | Home and Family | Tourism | Obituaries
Community |
Perspectives
|
Law & Courts |
Leisure Time
|
Spiritual Life |
Health & Fitness |
Teen Scene
Calendar
|
Letters to the Editor


 e fear of missing something weighs heavily on every doctor's mind. But the stakes are highest in the ER, and that fear often leads to extra blood tests and imaging scans for what may be harmless chest pains, run-of-the-mill head bumps, and non-threatening stomachaches.
e fear of missing something weighs heavily on every doctor's mind. But the stakes are highest in the ER, and that fear often leads to extra blood tests and imaging scans for what may be harmless chest pains, run-of-the-mill head bumps, and non-threatening stomachaches.

