Disease of 1,000 faces shows how science is tackling immunity’s dark
side
[November 07, 2025]
By LAURAN NEERGAARD
Doctor after doctor misdiagnosed or shrugged off Ruth Wilson’s rashes,
swelling, fevers and severe pain for six years. She saved her life by
begging for one more test in an emergency room about to send her home,
again, without answers.
That last-ditch test found the Massachusetts woman’s kidneys were
failing. The culprit? Her immune system had been attacking her own body
all that time and nobody caught it.
“I just wish there was a better way that patients could get that
diagnosis without having to go through all of the pain and all of, like,
the dismissiveness and the gaslighting,” she said.
Wilson has lupus, nicknamed the disease of 1,000 faces for its variety
of symptoms — and her journey offers a snapshot of the dark side of the
immune system. Lupus is one of a rogues’ gallery of autoimmune diseases
that affect as many as 50 million Americans and millions more worldwide
– hard to treat, on the rise and one of medicine’s biggest mysteries.
Now, building on discoveries from cancer research and the COVID-19
pandemic, scientists are decoding the biology behind these debilitating
illnesses. They’re uncovering pathways that lead to different autoimmune
diseases and connections between seemingly unrelated ones – in hopes of
attacking the causes, not just the symptoms.
It's a daunting task. That friendly fire ravages nerves in multiple
sclerosis, inflames joints in rheumatoid arthritis, dries out the eyes
and mouth in Sjögren's disease, destroys insulin production in Type 1
diabetes, weakens muscles in myositis and myasthenia gravis — and in
lupus, it can cause body-wide havoc.

The list goes on: A new count from the National Institutes of Health
tallied 140 autoimmune conditions, many rare but altogether a leading
cause of chronic disease that’s often invisible.
“You look normal. People see you and they don’t think you have this
horrible disease,” said Wilson, 43, who balances her illness with
volunteering to help educate the public and even doctors about life with
lupus.
While there’s still an enormous amount to learn, recent steps have some
specialists daring to wonder if just maybe, ways to cure or prevent at
least some of these diseases are getting closer.
In dozens of clinical trials, scientists are harnessing some of
patients' own immune cells to wipe out wayward ones that fuel lupus and
a growing list of other diseases. It's called CAR-T therapy and early
results with these “living drugs” are promising. The first lupus patient
was treated in Germany in March 2021 and remains in drug-free remission,
the researchers said last month.
And a drug named teplizumab can delay the start of Type 1 diabetes
symptoms in people destined to get sick, buying some time before they’ll
need insulin. Citing that “tantalizing evidence,” the NIH’s new
five-year plan for autoimmune research — if it gets funded — urges
pursuing similar windows to intervene in other simmering diseases.
“This is probably the most exciting time that we’ve ever had to be in
autoimmunity,” said Dr. Amit Saxena, a rheumatologist at NYU Langone
Health.
Inside job
Your immune system has multiple overlapping ways to detect and attack
bacteria, viruses or other bad actors. That includes teaching key
soldiers -- T cells and antibody-producing B cells — how to distinguish
what’s foreign from what’s “you.”
It’s a delicate balancing act, especially considering germs sometimes
adapt features similar to human molecules so they can confuse and sneak
past immune defenses. And while the immune system has built-in
safeguards to curtail any misbehaving cells, autoimmune diseases set in
when the system gets off-kilter.
Numerous genes involved in different immune functions can make people
susceptible to common autoimmune diseases. That means if one family
member is sick, others may be at increased risk. Such genes can include
variants that once protected our ancestors from long-ago threats
including the Black Death but that today can translate into a
hyperactive immune system.

But “genes are not everything,” said Dr. Mariana Kaplan of NIH’s
National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Studies show if one identical twin develops an autoimmune disease, the
other isn't guaranteed to get sick. Non-genetic factors that trigger an
immune response play a big role, such as infections, certain medicines,
smoking, pollutants. In lupus, even a bad sunburn is suspect.
“At some point there is a second or third hit and the immune system
says, ‘That’s it, I can’t handle any more of these insults,’” said
Kaplan, who directs systemic autoimmunity research.
And women are more likely to get autoimmune diseases than men, maybe
because of estrogen or their extra X chromosome. That's especially
evident in lupus; women account for 90% of cases, often young ones like
Wilson.
Fainting spells and body-wide rashes began in her 20s and intensified
with two pregnancies. Youngsters in tow, she saw a variety of doctors
for fevers, swelling, joint and back pain until that fateful ER visit
when she requested a urine test.
Months of grueling treatment saved her kidneys. But over a decade later,
the Littleton, Massachusetts, woman still lives with daily pain from
lupus. Deep fatigue and brain fog — difficulty with concentrating,
short-term recall, multitasking — wax and wane.
Therapies have improved in recent years, from high-dose steroids and
drugs that broadly suppress the immune system to include additional
options that focus on specific molecules. Wilson gets a monthly
lupus-targeted IV treatment and takes about six daily medicines to calm
her overactive immune system and related symptoms.
Worse are what are called flares, when symptoms abruptly and markedly
worsen. For Wilson, they bring sudden high fevers, legs too swollen to
walk, more intense pain, lasting days to a week. They impact her job at
a medical lab and time with her husband, teen son and college-age
daughter.
“It’s not a bad life, it’s just a bad day,” she tells herself to get
through.

[to top of second column]
|

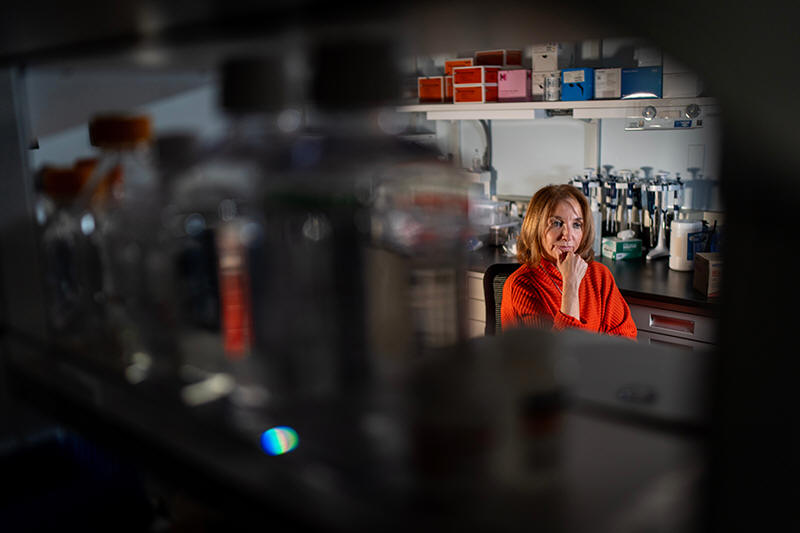
Dr. Mariana Kaplan, chief of the National Institute of Arthritis and
Musculoskeletal and Skin Diseases at the National Institutes of
Health, is photographed during an interview at her lab, Tuesday,
Jan. 21, 2025, in Washington. (AP Photo/David Goldman)
 Kaplan, the NIH scientist, has a
biological explanation for the daily slog: The same inflammatory
proteins that cause aches and fatigue during a cold or flu
continually course through the bodies of patients with systemic
autoimmune diseases like lupus.
Hunting the root causes
“These are my babies,” said Dr. Justin Kwong, a research fellow in
Kaplan’s lab at NIH, as he carefully examines cells in an incubator.
Kwong is performing something so tricky it's not done in many
laboratories: He's growing batches of neutrophils, the body’s most
common white blood cells.
They are first responders that race to the site of an injury or
infection, and Kaplan suspects they’re among the earliest immune
cells to run amok and trigger certain autoimmune diseases.
How? Some types of neutrophils spew out their insides to form sticky
spider-web like structures that trap and kill germs. The neutrophils
die in the process.
But patients with lupus and some other diseases harbor abnormal
neutrophils that form too many webs, Kaplan said. Her team is
investigating if other immune defenses mistakenly sense the
resulting debris as foreign, sparking a chain reaction.
“We think that’s a fundamental initial process,” Kaplan said. “We’re
trying to find why it happens, why it happens more often in women,
and can we come up with strategies to stop this without harming the
way we defend ourselves from infections.”
Another common feature: Patients with a number of autoimmune
diseases, especially women, often suffer heart attacks and strokes
at unusually young ages. Kaplan’s research suggests those aptly
named NETS, or neutrophil extracellular traps, may be key — by
damaging blood vessels and spurring hardened arteries typically seen
in older people.
But neutrophils don’t live long outside the body and testing mature
ones from lupus patients’ blood won’t show how they went awry —
something Kwong’s baby neutrophils may aid.

Teasing apart patient differences
Whatever triggers it, lupus has bafflingly varied symptoms and
treatments that can keep some patients symptom-free but not others.
That suggests “lupus is not a single disease,” Kaplan said. “What we
call lupus probably represents many different conditions that have
some common factors."
How to subtype lupus isn't clear. But another disease, rheumatoid
arthritis, may offer clues. Perhaps best recognized by painfully
disfigured fingers, RA can attack any joint and even some organs,
sometimes scarring lungs.
Like with lupus, RA treatment is trial-and-error and scientists are
exploring different underlying factors to explain why. In one study,
an international team used tiny samples of patients' joint tissue to
identify six inflammatory subtypes of RA based on patterns of cells,
how they clustered and their activity.
It “changed how we think about the disease,” said Northwestern
University rheumatology chief Harris Perlman, one of the coauthors.
Now researchers are comparing cells in joint tissue before and after
patients start a new drug to see if they could help guide treatment
choices, he said.
Living with lupus
Wilson learned to wear sunscreen and a big hat outdoors and how to
ration her energy in hopes of avoiding flares. When her kids were
old enough for school, she returned, too, getting degrees that led
to laboratory research and data science jobs — and a better
understanding of her own disease and its treatments.
One day her then-rheumatologist asked if she'd answer some medical
students' questions. Wilson remembers many knew “what lupus looks
like in a textbook” but not the patient perspective.
“I realized, my god, I need to start talking about this.”
What that looks like now: One evening last February, Wilson bubbled
with nerves and excitement at finally meeting some members of her
online lupus support group. At UMass Chan Medical School, Wilson
greeted the two women and two men with hugs. They shared symptoms
and treatments — and rueful stories of well-meaning relatives urging
them to just get more sleep to combat the lupus fatigue that rest
can't conquer.
A month later, Wilson traveled to Washington for a meeting organized
by the Lupus Research Alliance, where she urged scientists and drug
company researchers to heed patient reports of changes in their
everyday lives, such as whether a new therapy helps brain fog.
Drug studies that measure physical symptoms and blood markers are
“only capturing half the story,” she said. “If a treatment allows me
to think clearly, to engage in my life, to be the person I know I am
beneath all of this, then that is just as important as reducing
inflammation.”
While her doctor isn't recommending experimental treatments yet,
Wilson recently joined the Lupus Landmark Study that will track
biological samples from 3,500 patients to better understand disease
variations. Whenever a flare strikes Wilson pricks her finger for a
blood sample to share.
“It’s important for me to also be a voice for patients because I
think of myself and how lonely I was at the very beginning,” Wilson
said. For a long time, “I never wanted to talk about it. Especially
my kids, I wanted them to know that I was going to be OK. And so you
put on your makeup and your lipstick and your three shades of eye
corrector and you go on.”
All contents © copyright 2025 Associated Press. All rights reserved |